
FUNCTIONAL MOVEMENT SCREEN
Developed by Gray Cook, P.T. some 20 years ago, Functional Movement Screen (FMS) is a ranking and grading system created to document movement patterns that are key to normal function. By screening these patterns, functional limitations and asymmetries are readily identified. Basic movement pattern limitations can reduce the effects of functional training, physical conditioning, and distort proprioception (body awareness).

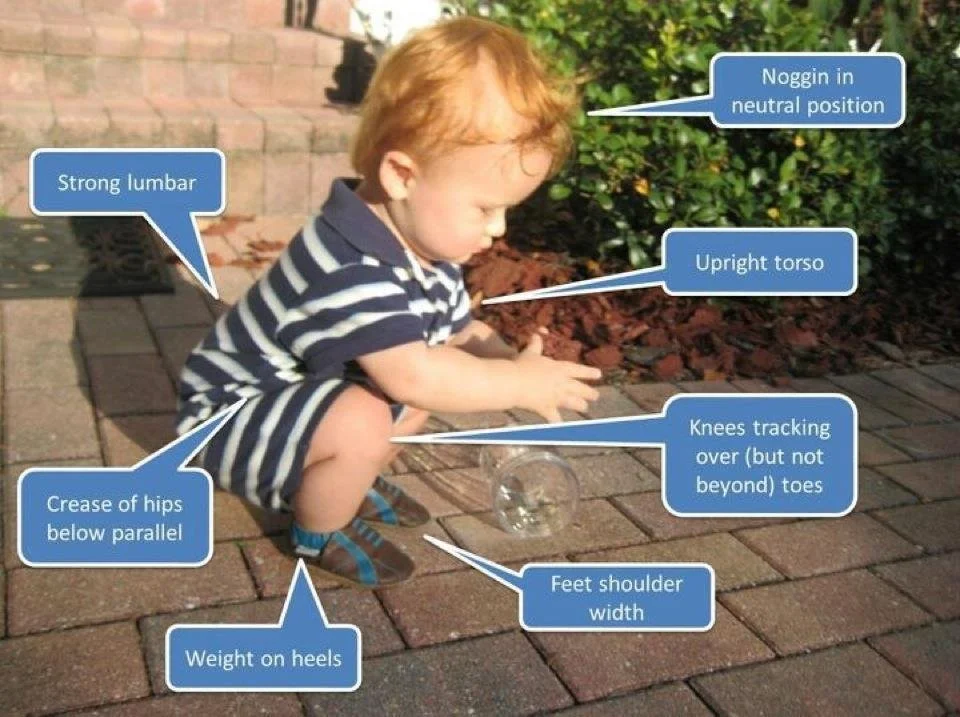
Simply stated, we are all born with the ability to carry out basic movement patterns and as we age those movements change. As a result, we develop “dysfunctional patterns” that can lead to pain and/or injury over time. A good example is if you look at a typical three-year-old child they are able to squat without any difficulty. (See image).
However, if we were to compare that to a 30-year-old who would not be able to come close to that position, what is the difference? Is it that the older person is out of shape, or simply not flexible enough? The answer is that they have developed “faulty movement patterns” that have led to some areas of the body lacking mobility and other areas lacking stability. FMS is a way of testing one’s weaknesses and then developing a customized “corrective exercise” program which is done 3/week. The program is carried out for 4-6 weeks and the individual is re-tested. This system is used by many professional and collegiate sports teams, including the N.Y. Giants. It is the product of an exercise philosophy based on sound science, years of innovation, and current research.
The benefits of FMS are widespread and can help anyone from an elite athlete to a weekend warrior. It is applicable to someone who may have had many different conditions treated just to have it happen again.
Consider, for example, a tennis player who has recurrent ankle sprains. They are treated appropriately with therapy and heal within a few weeks. Then they are given strengthening exercises and perhaps even got to physical therapy to carry them out. They are discharged with full range of motion and strength only to have it recur six months later. This scenario is all too common. “Thinking outside the box” allows us to look at this patient from a different perspective. Perhaps the issue is that they cannot do an “in line lunge,” due to instability. This person could do their standard stretching and strengthening exercises religiously and never really address the bottom line! On the other hand, if the underlying instability is identified and corrective exercises are done they will be less likely to sprain their ankle again.
This is a revolutionary way to avoid the injuries that 50% of our youth athletes deal with on a daily basis. How many times have you heard of baseball players being side-lined with shoulder or elbow injuries? New research suggests that in fact the curveball is not the culprit we once thought it was. Throwing a fastball or a curveball carries the same risk for injury. However, these studies were biomechanical in nature and don’t consider that the shoulder and elbow are not as stable as they are with a fastball. Doesn’t it follow then that one would want to measure the stability and flexibility of the shoulder and elbow to be sure that they are not already at a disadvantage due to dysfunction?
